

What Is Emergency Contraception?
Even with all of the different contraceptives and abortifacients on the market today, women forget to use their birth control, think their birth control method might have failed, or were coerced into sex.
Many of these women resort to “emergency contraception,” a term that covers several drugs or devices that are used after intercourse (instead of before) to avoid pregnancy. EC can take several forms. The most common are:
- The morning-after pill (MAP)
- Doubling up on birth control pills
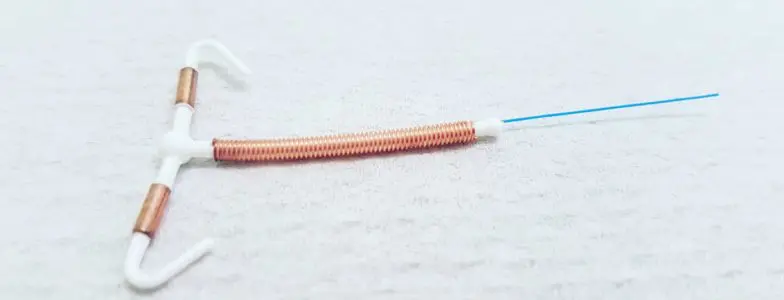
- Insertion of the Copper-T, or ParaGard intrauterine device.
The abortion drug mifepristone (RU-486) can also be used as emergency contraception.

Other drugs, including Meloxicam, Indocin and Ranitidin (normally used for pain, inflammation control and acid reflux, respectively) are under investigation for potential use as emergency contraception.
To begin with, the very term “emergency contraception” is inaccurate. It is another attempt to erase the distinction between true contraceptive and abortifacient action. When pro-lifers hear terms like “emergency postcoital contraception,” they can be sure that what is being discussed is an abortifacient cocktail.
1. Morning-After Pills
The term “morning-after pill” is also a misnomer, since these methods are most effective when used immediately after intercourse. There are three types of MAP:1
- Those that use the same hormones (estrogen and progestin) that are used in standard birth control pills, but in higher doses. These are specifically intended to be taken after intercourse instead of before, and are available without a prescription to anyone 17 years of age or older. Wyeth’s Ovral is the only MAP of this type, and consists of four tablets containing both the progestin norgestrel and synthetic estrogen in the form of ethinyl estradiol.
- Progestin-only (levonorgestrel) pills, known by the brand names Plan B and its generic equivalent Next Choice. These contain either a single 1.5 mg dose of LNG or two doses of 0.75 mg LNG each, taken 12 hours apart within 72 hours of intercourse. Barr Laboratories’ patient information insert for Plan B says that its product “… may inhibit implantation (by altering the endometrium). It is not effective once the process of implantation has begun.”
- Anti-progestin pills. These go by the brand names Duprisal 30, ella, ellaOne, Ulapristal 30 and UPRIS, and contain ulipristal acetate. They are available by prescription only and are effective for up to five days after intercourse.
2. Doubling Up on Birth Control Pills
The second type of emergency contraception consists of taking several doses of standard combined birth control pills that contain both progestins and synthetic estrogen. The Food and Drug Administration has determined that 26 brands of birth control pill, including Alesse, Levlen, Lo/Ovral Nordette, Ovral, Tri-Levlen and Triphasil are safe for use in what is sometimes called the “Yuzpe Regimen.”
3. IUDs
Finally, there are the IUDs. Paragard is the only non-hormonal copper intrauterine device used in the United States today. It releases copper ions that are toxic to both gametes (sperm and ovum) and decreases the probability of fertilization. The copper ions are also toxic to the very early embryo, either killing it or preventing it from implanting. Paragard can be inserted up to five days after intercourse to prevent a continuing pregnancy.
All forms of emergency contraception are abortifacient in nature. This is clearly specified on all of the patient information leaflets issued by their manufacturers. However, the mainstream media can always be depended upon to deliver misinformation to the public. For example, the New York Times has claimed, “Studies have not established that emergency contraceptive pills prevent fertilized eggs from implanting in the womb, leading scientists say.”
Since the medical profession switched the definition of “conception” from fertilization to implantation in the mid-1960s for the sole purpose of paving the way for new abortifacients, doctors do not believe they are misleading the public when they claim that “emergency contraception” does not cause abortions. Contraceptive Technology Update states, “MAP does not cause an abortion … RU 486 is different from MAP as it us used later and causes an already implanted ovum/embryo to detach from the uterine lining, which is why it has been called the “abortion pill”” [emphasis in original].1
The population control group Academy for Educational Development used the tried-and-true tactic of promising us the moon and the stars when it said, “Because almost half of all unintended pregnancies in the United States end in abortion, EC could therefore eliminate half of all abortions. … Using ECPs within 5 days of unprotected sex cannot result in abortion because pregnancy has not begun. And again, if ECPs are taken after implantation, the pregnancy will not be interrupted.”2
Catholicism and Emergency Contraception
Questions have arisen as to whether Catholic hospitals should administer emergency contraception to rape victims.
On this topic, the United States Conference of Catholic Bishops has written:
A female who has been raped should be able to defend herself against a potential conception from the sexual assault. If, after appropriate testing, there is no evidence that conception has occurred already, she may be treated with medications that would prevent ovulation, sperm capacitation, or fertilization. It is not permissible, however, to initiate or to recommend treatments that have as their purpose or direct effect the removal, destruction, or interference with the implantation of a fertilized ovum.
In other words, Catholic doctors may administer a medication to rape victims that has a contraceptive, but not an abortifacient, effect.

The problem here is that we cannot know for certain whether or not a woman who has been raped has already conceived. Current available technology in the form of pregnancy tests, including luteinizing hormone protocols and ovulation tests, cannot reliably provide this information after fertilization and before implantation. They can only inform us that implantation has taken place. By then, of course, emergency contraception would not work to end the pregnancy.
We have seen that all abortifacient methods (including all forms of emergency contraception) have multiple mechanisms of action, as clearly defined in Paragraph 12.1 of the standardized “Highlights of Prescribing Information” forms required by the Food and Drug Administration. One of these modes of action is alteration of the endometrium, thus making implantation impossible or difficult. In fact, no birth control drug exists that has a purely contraceptive mode of action. Therefore, whenever these pills are taken, or a Copper-T IUD is inserted after sexual activity, there is a significant risk that a new human life will be destroyed.
One of the necessities of good moral judgment is good scientific facts. If the facts are in doubt, then the safest course of action must conform only to the verifiable facts. In this case, when uncertainty injects itself, the safest course of action must be taken, even if this means doing nothing.
This principle led to the Pontifical Academy for Life issuing an October 2000 statement that stated, “From the ethical standpoint, the same absolute unlawfulness of abortifacient procedures also applies to distributing, prescribing and taking the morning-after pill. All who, whether sharing the intention or not, directly cooperate with this procedure, are also morally responsible for it.”
Conclusion
We should therefore treat the abortifacient Plan B “morning-after pill” and so-called “emergency contraception” in the same manner as we would handle Depo-Provera, the birth control pill (OC), Norplant and the intrauterine device (IUD). All of these work a certain percentage of the time to end the life of the early developing human being and are therefore inadmissible.
Theologian Father Peter Damian Fehlner, North American Superior for the Franciscan Friars of the Immaculate from 1996 to 2002, clarified this point. He said that as long as there is doubt as to whether or EC is abortive, it may not be used. “The fact is, if we have any doubt about whether a given action would directly risk someone’s life, entail a violation of justice or threaten the salvation of a soul, we may not act on the basis of a scientific probability. That means even if the pill in Plan B is only ‘dubiously’ abortive, we simply may not use it at all.”3
+ Endnotes
[1] “Ask Your Clinician… ” Contraceptive Technology Update, November 1995, page 141.
[2] Academy for Educational Development. “Building Emergency Contraception Awareness Among Adolescents: A Toolkit for Schools and Community-Based Organizations.” 2003, page 8. Others have made the same promise; see Mary Ann Marshall. “Morning Becomes Prophylactic.” Ms. Magazine, August/September 1999, pages 40 and 41.
[3] For an in-depth discussion of EC administration to rape victims at Catholic hospitals, see “Scientific Certitude, Moral Certitude, and Plan B.” The National Catholic Bioethics Quarterly, Winter 2011, pages 7 to 11. Also see Human Life International’s Truth and Charity Forum. “When in Doubt, Choose Life.”
Related Content










Dr. Brian Clowes has been HLI’s director of research since 1995 and is one of the most accomplished and respected intellectuals in the international pro-life movement. Best known as author of the most exhaustive pro-life informational resource volume The Facts of Life, and for his Pro-Life Basic Training Course, Brian is the author of nine books and over 500 scholarly and popular articles, and has traveled to 70 countries on six continents as a pro-life speaker, educator and trainer.